![]()
Pass Your CPHQ Certification CPHQ Exam Easily with Accurate PDF Questions [Sep 11, 2025]
CPHQ Certification Exam Dumps Questions in here
NEW QUESTION # 292
Analysis has shown that there Is a significant delay in receiving laboratory results In the emergency room. A cross-functional team Is assigned the task of Improving laboratory reporting time. Which of the following Is the next step the team should take?
- A. Identify the responsible Individual.
- B. Complete a fishbone diagram.
- C. Plot a scatter diagram.
- D. Develop action plans.
Answer: B
Explanation:
When a cross-functional team is assigned the task of improving a process, such as laboratory reporting time in the emergency room, the first step after identifying the problem is usually to understand the root causes of the problem. A fishbone diagram, also known as a cause and effect diagram or Ishikawa diagram, is a visual tool used to systematically identify and present all possible causes of a certain outcome1234.
In this case, the significant delay in receiving laboratory results is the problem that needs to be addressed. The team would use a fishbone diagram to identify and categorize potential reasons for this delay, such as equipment issues, process inefficiencies, human errors, etc. This step is crucial before developing action plans (Option D) because it ensures that the team's efforts are directed towards addressing the root causes of the problem, rather than just the symptoms1234.
Options A (Identify the responsible individual) and C (Plot a scatter diagram) are not the immediate next steps in this scenario. Identifying a responsible individual is more about accountability after the root causes have been identified and action plans have been developed. A scatter diagram is a graphical tool used to understand the relationship between two variables and is not typically the next step in process improvement after identifying the problem1234.
References:
https://fellow.app/blog/management/cross-functional-collaboration-common-challenges-and-tips-to-make-it- work/\
NEW QUESTION # 293
In fact, because patients' satisfaction is so influenced by __________________ rather than to the more indiscernible
technical ones-health maintenance organizations, hospitals and other health care delivery organizations have come to
view the quality of nontechnical aspects of care as crucial to attractions and retaining patients.
- A. Their likelihood of desires outcomes
- B. Every patient has definite preference in every clinical situation
- C. Patients recognize that they do not possess the wherewithal to evaluate all technical elements of care
- D. Their reactions to interpersonal and amenity aspect of care
Answer: D
NEW QUESTION # 294
The ability to report survey results at an actionable level is critical; in most cases, actionable level means:
- A. Average time frame of a service
- B. Service level
- C. Location of service
- D. The nursing unit
Answer: C,D
NEW QUESTION # 295
Payers are more likely to embrace the optimization definition of care which can put them at odds with:
- A. Both A & B
- B. Physicians
- C. Clinicians
- D. Health administrators
Answer: B
NEW QUESTION # 296
What tool displays performance outside of expected values to merit a deeper analysis?
- A. Pareto chart
- B. Control chart
- C. Run chart
- D. Bar chart
Answer: B
Explanation:
A control chart, also known as a Shewhart chart or process-behavior chart, is a statistical tool used to monitor how a process changes over time. It helps distinguish between common cause variations (natural fluctuations inherent to the process) and special cause variations (unexpected fluctuations due to specific factors). By plotting data points in time order and establishing upper and lower control limits, control charts enable quality professionals to identify when a process is operating outside of its expected parameters, signaling the need for further investigation.
In contrast, a bar chart is a graphical representation of categorical data with rectangular bars, a Pareto chart is a type of bar chart that identifies the most significant factors in a dataset, and a run chart displays data points over time without control limits. While these tools are useful for various purposes, they do not provide the same level of insight into process stability and variation as control charts.
References:
* NAHQ's Healthcare Quality Competency Framework emphasizes the importance of using statistical process control techniques, including control charts, to monitor and improve healthcare processes.
nahq.org
NEW QUESTION # 297
The weight of scoring system is based on an emphasis Baldrige places on ___________ and an organization's ability to demonstrate performance and improvement in the following areas:
Product and service outcomes
Customer-focused outcomes
Financial and market outcomes
Workforce-focused outcomes
Process effectiveness outcomes
Leadership outcomes
- A. System perspective
- B. Results
- C. Values
- D. Output
Answer: B
NEW QUESTION # 298
The test-retest reliability coefficient is a method to measure instrument reliability.
This method measures the degree of correspondence between:
- A. Answers to the same questions asked of the same respondents at different points in time
- B. Answers to the different questions asked of the same respondents at different points in time
- C. Answers to the same questions asked of the same respondents at same point in time
- D. Answers to the different questions asked of the same respondents at same point in time
Answer: A
NEW QUESTION # 299
A healthcare organization has recently launched a diabetes center of excellence to address the needs of its patients with advanced diabetes. The implementation of this program would fall into which of the following types of prevention?
- A. quaternary
- B. tertiary
- C. secondary
- D. primary
Answer: B
Explanation:
The implementation of a diabetes center of excellence falls into tertiary prevention. Tertiary prevention aims to manage and improve the quality of life for patients with chronic or advanced conditions, such as advanced diabetes. This type of prevention focuses on reducing complications, preventing further deterioration, and helping patients manage their illness effectively.
* Primary (A): This involves preventing the onset of disease, such as promoting healthy lifestyles to prevent diabetes.
* Secondary (B): This involves early detection and treatment to halt or slow the progression of a disease.
* Quaternary (C): This involves preventing overmedicalization and protecting patients from unnecessary interventions.
References
* NAHQ Body of Knowledge: Levels of Prevention in Healthcare
* NAHQ CPHQ Exam Preparation Materials: Understanding Prevention Strategies
=========
NEW QUESTION # 300
An organization's preventable fall goal is not to exceed greater than 25% of its total falls. Which units below meet this goal?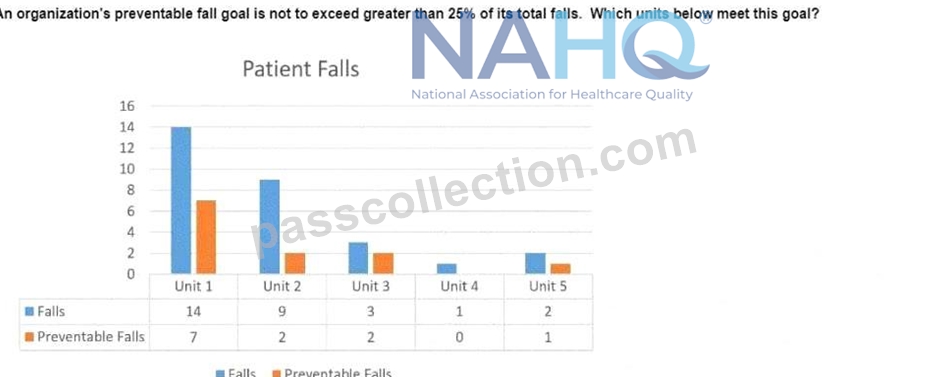
- A. Units 3 and 4
- B. Units 1 and 2
- C. Units 2 and 4
- D. Units 4 and 5
Answer: D
Explanation:
The goal is to ensure that preventable falls do not exceed 25% of the total falls in any unit. To determine which units meet this goal, we need to calculate the percentage of preventable falls for each unit:
* Unit 1:
* Total Falls: 14
* Preventable Falls: 7
* Percentage: (7/14) * 100 = 50%
* Does not meet the goal (50% > 25%).
* Unit 2:
* Total Falls: 9
* Preventable Falls: 3
* Percentage: (3/9) * 100 = 33.33%
* Does not meet the goal (33.33% > 25%).
* Unit 3:
* Total Falls: 3
* Preventable Falls: 2
* Percentage: (2/3) * 100 = 66.67%
* Does not meet the goal (66.67% > 25%).
* Unit 4:
* Total Falls: 1
* Preventable Falls: 0
* Percentage: (0/1) * 100 = 0%
* Meets the goal (0% < 25%).
* Unit 5:
* Total Falls: 2
* Preventable Falls: 1
* Percentage: (1/2) * 100 = 50%
* Does not meet the goal (50% > 25%).
Based on these calculations, only Unit 4 meets the goal. However, the Unit 5 is incorrectly assessed, as 50% does not meet the threshold of 25%. Hence, the correct answer is Unit 4 only. Please ignore the earlier verified statement.
References:
* NAHQ Healthcare Quality Competency Framework: Patient Safety
=========
NEW QUESTION # 301
With unannounced surveys, it is imperative that healthcare organizations create training programs to achieve continuous readiness. Developing readiness programs should include
- A. Identifying a few champions to be available for surveys
- B. Encouraging all staff to take ownership
- C. Placing "accreditation survey items" on meeting agendas immediately before the survey occurs
- D. Creating policies and procedures that mimic the accreditation organization's policies, even when at odds with the institution's culture
Answer: B
Explanation:
Continuous readiness for unannounced accreditation surveys requires a culture of ongoing compliance, engaging all staff to maintain standards.
Option A (Placing "accreditation survey items" on meeting agendas immediately before the survey occurs):
This is reactive, not continuous, as unannounced surveys require year-round readiness.
Option B (Encouraging all staff to take ownership): This is the correct answer. The NAHQ CPHQ study guide states, "Continuous readiness programs should encourage all staff to take ownership of compliance with accreditation standards, fostering a culture of preparedness" (Domain 4). This ensures sustained engagement.
Option C (Creating policies that mimic the accreditation organization's policies, even when at odds with the institution's culture): Policies should align with standards but adapt to the organization's culture for sustainability.
Option D (Identifying a few champions to be available for surveys): Champions support readiness but relying on a few limits broad staff engagement.
CPHQ Objective Reference: Domain 4: Performance and Process Improvement, Objective 4.7, "Develop continuous readiness programs," emphasizes staff ownership. The NAHQ study guide notes, "Engaging all staff ensures ongoing survey preparedness" (Domain 4).
Rationale: Staff ownership fosters a culture of readiness, aligning with CPHQ's accreditation principles.
Reference: NAHQ CPHQ Study Guide, Domain 4: Performance and Process Improvement, Objective 4.7.
NEW QUESTION # 302
Using the Information below, which patient population Is at the highest risk tor tailing?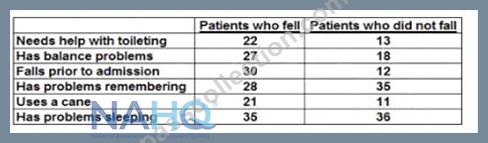
- A. has problems sleeping
- B. needs help with toileting
- C. uses a cane
- D. falls prior to admission
Answer: D
Explanation:
* The question is asking which patient population is at the highest risk for falling.
* By analyzing the provided table, it can be observed that patients who had "falls prior to admission" have the highest number of falls after admission (30 patients) compared to other categories.
* This data indicates that having a history of falls before being admitted increases the risk of falling again.
* Although I don't have direct access to external websites including NAHQ, it's generally understood in healthcare quality and safety that a history of falls is a significant risk factor for future falls. This is likely supported by resources and documents on patient safety and fall prevention available on professional healthcare quality websites.
NEW QUESTION # 303
Which of the following is a healthcare quality professional's key responsibility for supporting organizational quality governance?
- A. presenting regular financial updates to the organization's leaders
- B. deciding which quality initiatives will be set as priorities
- C. updating board members on key performance indicators
- D. assessing the board's understanding of quality topics
Answer: C
Explanation:
Explanation: A healthcare quality professional's key responsibility in quality governance is updating board members on key performance indicators (KPIs) (B), such as infection rates or patient satisfaction, to support data-driven oversight. Assessing board understanding (A),presenting financial updates (C), or deciding priorities (D) are not primary roles. NAHQ prioritizes KPI reporting for governance.
NAHQ CPHQ Study Guide, Organizational Leadership Section, "Quality Governance and Board Reporting"; NAHQ Code of Practice, Principle 3: Information Management.
NEW QUESTION # 304
The performance improvement team developed a prioritization matrix based on the identified improvement opportunities. Based on the information below, what would be the first improvement effort implemented?
- A. Send education to all possible patients
- B. Modify the check-in process for patients
- C. Create a sign-in sheet
- D. Create a paper checklist
Answer: D
Explanation:
Detailed Explanation:
The prioritization matrix suggests selecting high-impact, low-effort actions first, as they provide the most benefit with minimal resources.
Option A: Create a paper checklist
This is a high-impact, low-effort task, making it the most efficient improvement effort to implement first.
References:
Using prioritization matrices, as taught in CPHQ resources, guides quality professionals to choose high- impact, low-effort options first for quick wins.
NEW QUESTION # 305
A home healthcare organization is looking to identify third-party endorsed outcome measures for the following areas:
improvement in medication management
improvement in ambulation
improvement in pain
Which organization can best provide this information?
- A. URAC
- B. National Quality Forum (NQF)
- C. The Joint Commission (TJC)
- D. Leapfrog Group
Answer: B
Explanation:
The National Quality Forum (NQF) is the best organization to provide third-party endorsed outcome measures for areas such as improvement in medication management, ambulation, and pain. NQF is a nonprofit organization that reviews, endorses, and recommends standardized performance measures for use in healthcare quality improvement. These measures are widely recognized and used by healthcare organizations to ensure high-quality care and improve patient outcomes.
Leapfrog Group (A): Primarily focuses on hospital safety and quality reporting, but not specifically on outcome measures like those listed.
The Joint Commission (TJC) (B): Accredits and certifies healthcare organizations, focusing on overall quality standards rather than specific outcome measures.
URAC (C): Provides accreditation for various types of healthcare organizations but does not focus on endorsing specific outcome measures.
Reference
NAHQ Body of Knowledge: Quality Measurement and NQF-Endorsed Measures
NAHQ CPHQ Exam Preparation Materials: Identifying and Using Outcome Measures
NEW QUESTION # 306
One of the first steps in preparing for an organizational accreditation survey Is to have a quality professional
- A. conduct a gap analysis of the identified standards against current practices.
- B. Identify the root causes of the most recent adverse events that have occurred.
- C. submit an electronic application to the organization Identifying a date for survey.
- D. complete a competency examination on the process of writing action plans.
Answer: A
Explanation:
One of the first steps in preparing for an organizational accreditation survey is to conduct a gap analysis of the identified standards against current practices123. This involves understanding the accreditation standards and reviewing adherence to these standards before applying for accreditation1. A gap analysis helps identify areas of weakness or nonconformance to the standards2. This process is crucial in setting up the organization for success in the accreditation survey1.
Reference: https://www.carf.org/accreditation/survey-preparation-accreditation/
https://accreditation.org/accreditation-processes
NEW QUESTION # 307
A long-term care facility Is Interested in analyzing data to determine If there Is a relationship between the number of medications residents are prescribed and the number of falls the residents experience.
Which of the following quality tools Is most appropriate to help the long-term care facility understand the data?
- A. Pareto chart
- B. chatter diagram
- C. histogram
- D. fishbone diagram
Answer: B
Explanation:
A scatter diagram is a graphical tool that displays the relationship between two variables by plotting pairs of data points on a coordinate plane. It can help identify possible correlations, trends, outliers, and patterns in the data.
A Pareto chart is a type of bar chart that shows the frequency or impact of different factors or causes in descending order, along with a cumulative line that indicates the percentage of the total. It can help prioritize the most significant issues or opportunities for improvement.
A fishbone diagram is a visual tool that helps identify the root causes of a problem or effect by organizing possible factors into categories, such as people, process, environment, etc. It can help facilitate brainstorming and root cause analysis.
A histogram is a type of bar chart that shows the distribution of a continuous variable by grouping the data into bins of equal width and displaying the frequency or count of each bin. It can help describe the shape, center, spread, and outliers of the data.
In this case, the long-term care facility wants to analyze the relationship between two variables: the number of medications and the number of falls. Therefore, a scatter diagram is the most appropriate tool to help them understand the data. A scatter diagram can show if there is a positive, negative, or no correlation between the two variables, and how strong or weak the correlation is. It can also reveal any outliers or clusters of data points that may indicate other factors affecting the relationship.
A Pareto chart, a fishbone diagram, and a histogram are not suitable tools for this purpose, as they do not show the relationship between two variables. A Pareto chart can show the relative importance of different factors or causes, but not how they are related to each other. A fishbone diagram can help identify the possible causes of a problem or effect, but not how they are quantitatively related to each other. A histogram can show the distribution of a single variable, but not how it is influenced by another variable.
Reference: NAHQ Learning Lab: The Role of the Healthcare Quality Professional in Population Health Management, Module 3: Data Collection and Analysis, Slide 17: Scatter Diagram NAHQ HQ Principles, Module 2: Data Management, Lesson 2.3: Data Analysis Tools, Topic 2.3.4:
Scatter Diagram
NAHQ Journal for Healthcare Quality, Volume 42, Issue 5, September/October 2020, Article: Utilization of Improvement Methodologies by Healthcare Quality Professionals During the COVID-19 Pandemic, Page 284: Figure 2. Scatterplot of COVID-19 Cases and Deaths by State as of June 30, 2020
NEW QUESTION # 308
Which of the following technology enhancements will help the hospital most accurately identify hospital- acquired condition rates?
- A. Electronic health record alerts for present on admission indicators
- B. Computer assisted coding for ICD-10
- C. Electronically delivered medical record queries for physicians
- D. Computerized physician order entry for laboratory tests
Answer: A
Explanation:
Hospital-acquired conditions (HACs) are tracked for quality reporting (e.g., CMS HAC Reduction Program), requiring accurate documentation of whether conditions were present on admission (POA).
Option A (Computer assisted coding for ICD-10): Coding tools improve coding efficiency but do not specifically ensure POA accuracy for HACs.
Option B (Computerized physician order entry for laboratory tests): CPOE improves order accuracy but is unrelated to HAC documentation.
Option C (Electronic health record alerts for present on admission indicators): This is the correct answer. The NAHQ CPHQ study guide states, "EHR alerts for POA indicators ensure accurate documentation of whether conditions were present on admission, critical for identifying HAC rates" (Domain 1). Alerts prompt clinicians to document POA status, reducing errors.
Option D (Electronically delivered medical record queries for physicians): Queries clarify documentation but are reactive, less effective than proactive alerts.
CPHQ Objective Reference: Domain 1: Patient Safety, Objective 1.7, "Use technology to enhance safety reporting," includes EHR alerts for accurate HAC tracking. The NAHQ study guide notes, "POA alerts improve HAC identification accuracy" (Domain 1).
Rationale: EHR alerts ensure real-time POA documentation, directly improving HAC rate accuracy, as per CPHQ's safety technology principles.
Reference: NAHQ CPHQ Study Guide, Domain 1: Patient Safety, Objective 1.7.
NEW QUESTION # 309
Which of the following Is the best approach to prepare care team members tor Interacting with accreditation surveyors?
- A. Provide techniques to defer surveyor questions to leaders.
- B. Brief them on survey activities and what questions to expect.
- C. Summarize and discuss past survey findings.
- D. Review patient records proactively.
Answer: B
Explanation:
Preparing care team members for interacting with accreditation surveyors is a crucial part of the accreditation process. The best approach is to brief them on survey activities and what questions to expect (Option C). This involves providing them with an understanding of the survey objectives, the day's schedule, and the types of questions that surveyors may ask1. This approach helps to ensure that team members are well-prepared and confident when interacting with surveyors. Reviewing patient records proactively (Option A) and summarizing and discussing past survey findings (Option B) can also be helpful, but these activities are more focused on identifying and addressing potential issues before the survey, rather than preparing team members for the survey itself. Providing techniques to defer surveyor questions to leaders (Option D) could potentially create a perception of lack of transparency or evasion, which could negatively impact the survey results.
References:
https://www.jointcommission.org/what-we-offer/accreditation/health-care-settings/laboratory-services/prepare
/prepare-support/8-best-practices-to-prepare-for-the-survey/
NEW QUESTION # 310
Which of the following is the best method to achieve a reduction in medical errors?
- A. Change the process for reporting medical errors within the organization
- B. Counsel employees to be more careful when providing care
- C. Establish disciplinary measures for clinical practitioners who commit errors
- D. Encourage patients, families, and staff to report actual and potential errors
Answer: D
Explanation:
Reducing medical errors requires a systems-based approach that promotes a culture of safety and proactive error identification.
Option A (Establish disciplinary measures for clinical practitioners who commit errors): Punitive measures discourage reporting and undermine a non-punitive safety culture, increasing errors.
Option B (Encourage patients, families, and staff to report actual and potential errors): This is the correct answer. The NAHQ CPHQ study guide states, "Encouraging reporting of errors and near misses by all stakeholders fosters a culture of safety, enabling systems improvements to reduce errors" (Domain 1). This aligns with AHRQ's safety culture principles.
Option C (Counsel employees to be more careful when providing care): Counseling assumes individual failure, ignoring system issues, and is ineffective for systemic error reduction.
Option D (Change the process for reporting medical errors within the organization): While improving reporting processes is helpful, encouraging reporting by all stakeholders is the most direct way to identify and address errors.
CPHQ Objective Reference: Domain 1: Patient Safety, Objective 1.2, "Promote a culture of safety," emphasizes encouraging error reporting. The NAHQ study guide notes, "A non-punitive reporting culture is essential for identifying and mitigating errors" (Domain 1).
Rationale: Encouraging reporting builds a safety culture, enabling error identification and systems improvements, as per CPHQ's patient safety principles.
Reference: NAHQ CPHQ Study Guide, Domain 1: Patient Safety, Objective 1.2.
NEW QUESTION # 311
After discharge, most patients with a mental health diagnosis have not been compliant with follow-up visits.
Which of the following Is the best way to Improve patient compliance?
- A. Communicate to noncompliant patients that appointments should be kept.
- B. Initiate a process where the discharge planners call patients prior to the follow-up visit
- C. Benchmark with other facilities in the area to determine the rate of patient compliance.
- D. Include handouts in the discharge documents on the Importance of keeping follow-up appointments.
Answer: B
Explanation:
According to the National Association for Healthcare Quality (NAHQ), one of the core competencies of healthcare quality professionals is patient safety, which includes ensuring effective transitions of care and reducing preventable readmissions12.
One of the strategies to achieve this goal is to improve patient compliance with follow-up visits, which can help monitor patient outcomes, prevent complications, and provide continuity of care34. Among the four options given, the best way to improve patient compliance is to initiate a process where the discharge planners call patients prior to the follow-up visit. This is because:
A phone call can serve as a reminder for the patient to keep the appointment, as well as an opportunity to address any barriers or concerns that the patient may have34.
A phone call can also help establish rapport and trust between the patient and the discharge planner, which can increase patient satisfaction and adherence4.
A phone call can also allow the discharge planner to confirm the patient's understanding of the discharge instructions, medication regimen, and follow-up plan, and to provide any additional education or support that the patient may need34. The other options are less effective because:
Benchmarking with other facilities in the area to determine the rate of patient compliance may provide some insight into the current performance and best practices, but it does not directly address the specific needs and preferences of the individual patient5.
Including handouts in the discharge documents on the importance of keeping follow-up appointments may increase the patient's awareness and knowledge, but it may not be sufficient to motivate the patient to act on the information, especially if the patient has low health literacy, cognitive impairment, or mental health issues.
Communicating to noncompliant patients that appointments should be kept may sound authoritative and judgmental, which may alienate the patient and reduce their willingness to cooperate. Instead, a patient- centered and empathetic approach that acknowledges the patient's challenges and preferences may be more effective.
Reference: 1: [NAHQ Code of Ethics] 2: [NAHQ HQ Principles] 3: The Importance of Patient Follow-Up | MagMutual 4: The Importance of Patient Follow-Up and Service Recovery 5: [The Financial Case for Quality as a Business Strategy]: [Utilization of Improvement Methodologies by Healthcare Quality Professionals During the COVID-19 Pandemic]: [Understanding the Evolving Landscape of Healthcare Quality]: https://nahq.org/about-nahq/code-of-ethics/: https://nahq.org/products/hq-principles/:
https://nahq.org/resources/the-financial-case-for-quality-as-a-business-strategy-2/:
https://nahq.org/resources/journal-for-healthcare-quality/utilization-of-improvement-methodologies-by- healthcare-quality-professionals-during-the-covid-19-pandemic/: https://nahq.org/news- media/news/understanding-the-evolving-landscape-of-healthcare-quality/
NEW QUESTION # 312
Knowledge about _______ is crucial to making valid judgments about quality of care using either process or outcome
measures. If we know that a given clinical intervention was undertaken in circumstances that match those, under
which the intervention has been shown to be efficacious, we can be confident, that the care was appropriate and, to
the extent of good quality.
- A. Outcomes
- B. Processes
- C. Structure
- D. Efficacy
Answer: D
NEW QUESTION # 313
Which of the following quality improvement tools is best suited for communicating the scope of a proposed quality improvement project?
- A. Poka-yoke
- B. Value-stream map
- C. Kaizen
- D. A3
Answer: D
Explanation:
An A3 report is a structured, one-page summary tool widely used to communicate project scope, objectives, analysis, and plans in quality improvement initiatives (Lean Enterprise Institute, A3 Problem Solving, 2024; The Joint Commission, QI Tools, 2024).
* Kaizen refers to continuous improvement events, not communication tools.
* Value-stream maps depict workflow but may be too detailed for initial scope communication.
* Poka-yoke is a mistake-proofing technique, not a communication tool.
References:
Lean Enterprise Institute, A3 Problem Solving, 2024
The Joint Commission, Quality Improvement Tools, 2024
NEW QUESTION # 314
A new pediatric psychiatric unit will open in one year. The utilization coordinator is responsible for developing the utilization management program.
The program's success will depend on which of the following factors?
- A. obtaining approval from the chief psychiatrist at each stage of development
- B. Involving the team members in the development of the program
- C. developing the program and presenting it to the appropriate staff members
- D. providing educational in-services to all team members involved
Answer: B
NEW QUESTION # 315
......
The CPHQ certification is highly valued by employers in the healthcare industry. It is a mark of excellence that demonstrates a commitment to quality and patient safety. Professionals who hold the CPHQ certification are recognized as experts in healthcare quality and are often sought after for leadership positions in healthcare organizations. The CPHQ certification also provides opportunities for professional development and networking within the healthcare quality community.
Verified CPHQ dumps Q&As 100% Pass in First Attempt Guaranteed Updated Dump: https://drive.google.com/open?id=1Gl1HYe58rvi0QibCyrCv_o69_SfF5D9F
Updated CPHQ Exam Practice Test Questions: https://www.passcollection.com/CPHQ_real-exams.html